The term PCT (Post Cycle Therapy), as we well know, refers to the phase that follows the end of the AAS cycle. Since AAS causes a temporary suppression of HPTA axis function and hence the synthesis of endogenous androgens, this is a problem that should be diligently addressed at the end of the cycle. If AAS stops suddenly without adequate support procedures for HPTA regeneration (as well as control of cortisol and excess estrogen in the blood), the result may be a long-term state of hypogonadism (low androgen levels), characterized by significant muscle loss, decreased energy levels, depression, decreased libido , sexual dysfunction, fat accumulation and gynecomastia. Many bodybuilders refer to this condition as the Post-Crash Cycle.
In the human body, the hypothalamus-pituitary-gonadal axis (HPTA) controls the biosynthesis of testosterone. HPTA is a highly regulated system that works to ensure and maintain the correct testosterone levels. This regulatory process is divided into three levels:
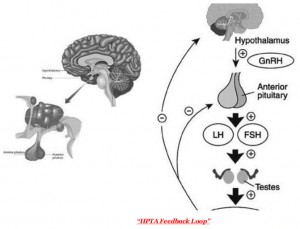
- At the top is an area of the hypothalamus of the brain that releases GnRH ( Gonadotropin Releasing Hormone ) when it detects a need to increase testosterone synthesis.
- GnRH sends a signal to a second level of the axis, the pituitary gland, to produce luteinizing hormone (LH).
- LH, in turn, sends a message to the Leydig cells in the testes, which will secrete testosterone.
 Given this role, LH is considered to be the primary messenger for controlling testosterone synthesis. Testosterone and other sex steroids, which are produced as a result of LH stimulation, act as a counterbalance. They provide negative feedback to reduce LH and testosterone secretion while preventing overproduction. Synthetic anabolic steroids, of course, send the same negative responses.
Given this role, LH is considered to be the primary messenger for controlling testosterone synthesis. Testosterone and other sex steroids, which are produced as a result of LH stimulation, act as a counterbalance. They provide negative feedback to reduce LH and testosterone secretion while preventing overproduction. Synthetic anabolic steroids, of course, send the same negative responses.
The release of GnRH (gonadotropin releasing hormone) by the hypothalamus stimulates the pituitary gland to release luteinizing hormone (LH) and follicle stimulating hormone (FSH). This (LH) promotes the release of testosterone from the testes. Androgens, as well as estrogens and progestins, in turn induce negative feedback from the hypothalamus and pituitary gland, decreasing the production of gonadotropins and testosterone when too much hormone is present.
Unsupported HPTA Recovery
Suppression of natural testosterone synthesis with steroid use is usually temporary. Even if you don’t do anything, normal endogenous androgen synthesis resumes a couple of months after your cycle ends. The problem is that during this period, adequate testosterone production with adequate cortisol control helps maintain muscle tissue. Most of the muscle gained from taking AAS can be easily lost in the weeks and months that follow if low androgen levels decline. PCT is widely used by bodybuilders and athletes to stimulate HPTA, thereby normalizing androgen production levels more quickly.
Measurement of LH and testosterone levels one week after the last injection of 250 mg testosterone enanthate. Note that between weeks 1 and 5, testosterone levels decline due to the cessation of exogenous androgen administration, while LH levels begin to adjust. From 5 to 10 weeks, testosterone levels begin to adjust. From weeks 5 to 10, testosterone levels remain very close to baseline, although LH levels increase from that point. There are no significant adjustments to testosterone levels until week 10. There is no research on the aspect of post-use anabolic steroid use, especially in AAS abusers. In most cases, mention should be made of monotherapy studies, usually in patients undergoing hormone replacement therapy. One of the most detailed studies on the hormonal situation after AAS has been done using testosterone enanthate. The study included a group of men who were given 250 mg of testosterone enanthate weekly for 21 weeks, which is certainly a higher dose than that commonly used for HRT. Various hormones were measured every week during the study and for more than 4 months after the drug was stopped. A review of the data shows that at the start of the study, LH levels were suppressed in direct association with increased testosterone levels (see Figure opposite). However, after discontinuing the steroid, there was a delay between the return to normal LH production (which began to correct from week 3) and testosterone (which took more than 10 weeks to clear corrective levels).
The above study suggests that one of the first things that happens after the AAS stops is that the brain recognizes that testosterone levels are low. This will cause the GnRH and LH levels to start correcting quickly enough. The significant delay between this and the increase in testosterone levels is largely due to the insensitivity of the testes to luteinizing hormone.
After a few months of receiving the stimulus, their activity is extremely weak and their size will decrease (atrophy). This is a well-documented side effect of anabolic steroid use, although the difference in size may not be noticeable in all cases. When LH levels begin to rise, the testes initially cannot handle the workload. This is expected to improve over time, but it may take several weeks for the testes to slowly regain their original size and activity. Since much of the post-cycle recovery period is actually characterized by normal (even low) LH levels, we should expect recovery if we expect it to be effective.
PCT doctor program. Scully
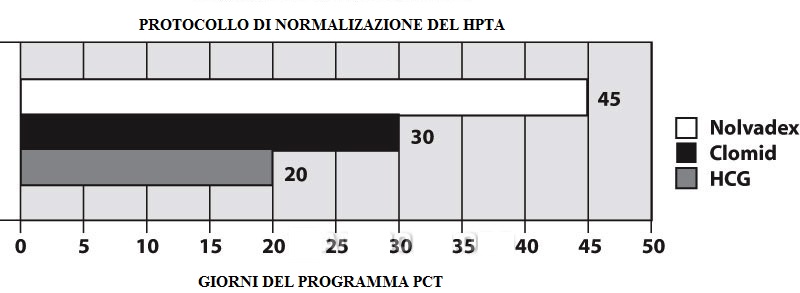
The following PCT program was developed by Dr. Michael Scali, one of the most renowned and respected experts in the field of anabolic steroids and the medical use of hormone replacement therapy for men. Scali has exerted particularly strong pressure in the medical community and government to acknowledge the hormonal imbalance following steroid use, which he called anabolic steroid-induced hypogonadism (ASIH). He has also performed blood tests on hundreds of patients and developed the following PCT program. A slightly modified form of this program was outlined in a clinical report of 19 healthy men taking supraphysiological (highly suppressive) doses of testosterone cypionate and nandrolone decanoate for 12 weeks. Scally’s HPGA Normalization Protocol focuses on the combined use of HCG, Nolvadex and Clomid and is arguably the largest and most clinically supported post-cycle therapy program currently available.
This PCT program starts with a significant dose of hCG (2000 IU every other day for 20 days). Tamoxifen citrate (20 mg twice daily) and clomiphene citrate (50 mg twice daily) are used. Clomid is used for 30 days. While the use of this class of antiestrogens may not be very effective in the first couple of weeks, it should be more critical towards the middle and end of the program.
In the published version of the Scally program (which is slightly modified) Based on the above), normal hormonal function returns to all subjects within 45 days. This is a clear success, far more favorable than the long recovery period reported in the study with 250 mg of testosterone enanthate per week.
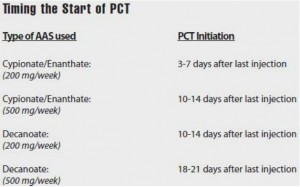
Keeping the correct timing for starting a post-cycle therapy program can be just as important as its composition. If it started too late, circulating AAS would drop excessively, resulting in a sudden loss of muscle mass gained during the cycle. If you run the program too early, you may lose your window of optimal performance.
The 20-day period of time during which hCG is used is most critical. In particular, we want to make sure that hCG is applied during the period when exogenous steroids fall below the physiological threshold of androgenic stimulation. In the case of testosterone (it’s easier to understand and explain the molecule), this will happen before the blood level falls below the normal level (350 ng / dL). There should be little overlap with cycle time so that hCG has a short period of time to work before AAS levels drop dramatically. 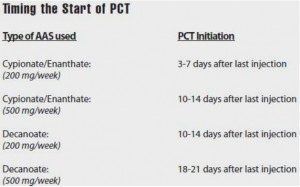 The exact time to start a PCT program is determined by the half-life of the drug used. We will use Testosterone Cypionate / Enanthate as an example. We know that each injection has a half-life of about 8 days. A dosage of 200 mg per week should result in a blood level threshold of around 2000-2400 ng / dL after several weeks of use. It will take about 3 weeks (24 days) for testosterone levels to drop to 250-300 ng / dL at this dosage. Thus, the PCT program should begin a few days to a week after the last testosterone injection. The start of the program may be delayed at higher doses. For example, at 500 mg per week T.C./T.E. It takes about 4 weeks (32 days) for testosterone to drop below normal levels. In this case, PCT will begin about two weeks after the last testosterone injection. For an oral PCT cycle, start 7-10 days before the last dose.
The exact time to start a PCT program is determined by the half-life of the drug used. We will use Testosterone Cypionate / Enanthate as an example. We know that each injection has a half-life of about 8 days. A dosage of 200 mg per week should result in a blood level threshold of around 2000-2400 ng / dL after several weeks of use. It will take about 3 weeks (24 days) for testosterone levels to drop to 250-300 ng / dL at this dosage. Thus, the PCT program should begin a few days to a week after the last testosterone injection. The start of the program may be delayed at higher doses. For example, at 500 mg per week T.C./T.E. It takes about 4 weeks (32 days) for testosterone to drop below normal levels. In this case, PCT will begin about two weeks after the last testosterone injection. For an oral PCT cycle, start 7-10 days before the last dose.