This article is in no way intended to encourage the use of currently prohibited substances, the content contained therein does not represent / replace a medical prescription, but has only the noble intention of providing FREE INFORMATION. The blog and the author are exempt from any liability.
________
 As an endocrinology student, nutritional scientist since 2005, and fitness enthusiast, I write articles on nutrition, education and many more devoted to an extremely detailed discussion of anabolic steroids and performance medications. I decided to write a short “tutorial” needed to use anabolic steroids / drugs. My friends and colleagues keep asking me why I keep learning about anabolic / androgenic steroids (AAS) and performance enhancing drugs. After all, the AAS are still demonized and, since the substances are under control, are inherently illegal. As a result, as an “advocate” of anabolic steroids, I am often criticized and targeted by drug dealers. Of course, the AAS issue will not be a popular topic of discussion in family gatherings!
As an endocrinology student, nutritional scientist since 2005, and fitness enthusiast, I write articles on nutrition, education and many more devoted to an extremely detailed discussion of anabolic steroids and performance medications. I decided to write a short “tutorial” needed to use anabolic steroids / drugs. My friends and colleagues keep asking me why I keep learning about anabolic / androgenic steroids (AAS) and performance enhancing drugs. After all, the AAS are still demonized and, since the substances are under control, are inherently illegal. As a result, as an “advocate” of anabolic steroids, I am often criticized and targeted by drug dealers. Of course, the AAS issue will not be a popular topic of discussion in family gatherings!
– Why go on talking about their uses and effects then? –
– Why am I so interested in the truth about AAS? –
– Why deal with anabolic steroids? –
My answer is based on two main reasons:
- striving to minimize negative health effects of AAS users through a harm reduction / prevention approach;
- I want to talk about the important health benefits of proper use of AAS that have been neglected in the past by the medical community; These benefits are among the same effects that athletes improve.
I had no idea how controversial such an open discussion of AAS would be, or how inconvenient it would be for many people. Due to the subversive information about available AAS, I would like to devote some time to a little more thorough discussion of both of these reasons.
Philosophical approach to teaching drug use and drug abuse prevention
Undoubtedly, the success of traditional drug prevention programs. The main reason is the misconception that the use of any drug is harmful to health; hence, the (unattainable) goal of these approaches is complete abstinence from drugs. My approach to drug education has always been a harm reduction / prevention strategy.
Rather than preventing the use of steroids or other “doping” drugs, I think the most practical and feasible approach is to prevent the abuse of the same drugs. This approach recognizes the difference between drug use and drug abuse. You can use the drug without overusing it. No medicine, when used correctly, is inherently harmful, not even demonized anabolic steroids!
Knowledge is power, the more information is available to the consumer, the better the decisions he can make. The Internet has become an extremely effective way for me to disseminate information to consumers about anabolic steroids / drugs. I have provided comprehensive and truthful information, news and resources about AAS / medicines that are aimed at minimizing / preventing damage associated with its use.
– What is harm reduction / prevention? –
Therefore, harm reduction / prevention can include the following points:
- teach bodybuilders to use AAS / medications safely and responsibly,
- talk about contradictions in the use of AAS / medications, so as not to aggravate the associated health problems,
- teach bodybuilders to cycle AAS / drugs and avoid consistent use for extended periods of time
- inform athletes about the inhibition and restoration (PCT) of natural testosterone production,
- inform Bodybuilders of the lowest possible dose of AAS / drug sufficient to achieve the desired effect
- discuss the pharmacological differences between AAS / drugs available on the market
- teach correct injection techniques together with the importance of sterility of needles and syringes,
- train athletes to scrutinize the source of drugs by verifying their actual potency and purity (especially if they come from UGL on the black market)
- teach bodybuilders to do regular blood tests
- teach how to order farm correctly.
- teach bodybuilders to use supplements that maximize health protection while avoiding and limiting side effects (altered transaminases, altered blood lipids, etc.)
In short, it means doing everything possible to minimize the negative health effects of the AAS / drug user.
Despite the controversial nature of the harm reduction / prevention approach in the bodybuilding community, it is my duty to keep health at the center of my drug / AAS education efforts. I have always thought that a harm reduction / prevention approach would benefit most not only the bodybuilder and athlete who chooses to use AAS / drugs, but society as a whole.
Health Comes First
Any bodybuilder and athlete in general who decide to use AAS / medications should first monitor their overall health through periodic blood tests. Many athletes, especially amateurs or amateurs, forget this aspect, spending perhaps € 500 on an AAS / medication cycle, and not even € 10 on basic health signs! Which should never be underestimated.
For example, most oral AAS have methylation at the C-17 position, and this makes the molecule hepatotoxic. If an athlete decides to use an AAS protocol / drugs that exhibit this characteristic, or a similar one that causes stress in the liver, it is good that the person concerned regularly undergoes (depending on cycle length) special controls for transaminases so that they reach levels of change that indicate possible liver damage.
Changes usually persist for up to 2-3 weeks after stopping the drug, and then return to physiological levels. It should also be noted that blood tests in people are much worse after heavy drinking (the norm for many young people) than in someone who has taken large doses of Anadrol .; at the same time, I absolutely do not want to take away what was said earlier (use and not abuse drugs), but this is just what it is. However, if the liver is suffering from long-term damage, the athlete may forget to make progress in the future. To minimize these effects on the liver, there are commercially effective hepatoprotective supplements such as Testosterone, Silymarin (400-600 mg / day), NAC (1,2-2 g / day), tuda (250-750 mg / day), samyr (400-800 mg / day), etc.
Another factor that most often creates problems for the user is the change in blood lipids. Cycles with AAS methylated at C-17 or cycles with high doses of AAS for extended periods of time lead to a decrease in high density lipoprotein (HDL) cholesterol. This is mainly due to the effects on the liver of the molecules used (especially those methylated at C-17) and the decreased use of LDL cholesterol for the production of androgens, which is reduced or interrupted during the AAS cycle. HDL removes cholesterol from the blood and returns it to the liver. The liver breaks down cholesterol into bile and then removes it from the body. This is the only way to rid the body of excess cholesterol. This is not like fat that can be burned / oxidized. As a rule, little or no effects are observed with the use of nandrolones, if the weekly dose does not exceed 2.2 mg per kg of body weight. There are some studies that support the idea that nandrolones have a positive effect on HDL levels. Diet plays an important role in heart and heart health. A diet rich in monounsaturated fatty acids and essential fatty acids such as EPA, DHA, and GLA helps prevent heart rhythm disturbances and increases HDL levels by lowering LDL and triglyceride levels.
Any diet should limit saturated fat intake to 10-20% of total lipid intake per day. For high cholesterol levels, there is a prescription drug called Mevacor that contains lovastatin, which prevents the synthesis of cholesterol in the liver. It does this by inhibiting a specific liver enzyme (an enzyme that is altered when methylated AAS is taken at c-17). It is unfortunate, however, that this drug is causing liver and heart damage. Red rice naturally contains lovastatin and is a free product. 2.5-3 g per day has been shown to have similar effects with Mevacor. At higher doses, lovastatin can cause muscle damage. Coenzyme Q-10 appears to prevent this effect. Niacin also helps lower cholesterol levels and the associated negative problems. 300mg-3g per day (depending on the health of the athlete) has given excellent results in most users by increasing HDL and lowering LDL (niacin, like other B complex vitamins, can inhibit the use of fat as an energy source by stimulating the use of carbohydrates for this purpose). Guggulsterones are also used to help lower LDL cholesterol and triglycerides. 40-60 mg per day of pure extract worked well for this purpose.
Another problem that athletes usually face when using AAS is the increase in the number of red blood cells (hematocrit). AAS, with variations between different molecules, stimulates the kidneys to synthesize erythropoietin (EPO), which in turn stimulates the production of red blood cells. As you well know, Anadrol was prescribed clinically for this purpose. The increase in red blood cells increases oxygen transport, vascularity, filling and muscle consistency. From the point of view of the bodybuilder / athlete, this was somewhat positive. Having too many red blood cells for extended periods of time increases blood volume to a point that slows circulation. This increases the likelihood of blood clots forming and therefore also increases the likelihood of stroke and heart attacks. To prevent this, in cases where the problem may persist despite the use of high doses of omega-3s, or if blood tests show significant changes, the use of 100 mg / day cardio aspirin is recommended. The most influential AAS in this sense are Boldenone, Oxymetholone https://steroide24.com/shop/orale-steroide/oxymetholon.
AAS also cause activation of the renin-angiotensin system in the kidneys. This, in turn, promotes the secretion of aldosterone by the adrenal glands, which leads to water retention, which can lead to high blood pressure or hypertension. Aldosterone is a hormone that helps maintain blood volume by increasing sodium retention and therefore water retention. Increasing water retention increases blood pressure in the heart, and if the situation persists for too long, heart disease can occur. An excessive increase in estrogen (depending on the molecule used) also causes water retention and the problems described above; but this topic deserves further study. However, drugs such as cyclic diuretics (Lasix) or potassium-sparing drugs (Moduretic) or special drugs such as clonidine hydrochloride (Catapres) are available to prevent / limit this problem. Given the dangers of these substances, especially when used by novices and without the supervision of a physician / expert, fortunately, they can be rolled up on very effective over-the-counter products such as dandelion (diuretic, natural potassium) that has shown excellent efficacy in a (divided) dose 300-600 mg per day.
An uncontrolled increase in estrogen levels is also a cause of anxiety for the athlete, as well as the cause of many of the factors mentioned above and others, such as fat accumulation in the female model and gynecomastia. There are several prescription drugs available to solve the problem with different functions than estrogens:
- antagonists : They are molecules that act as antagonists of the estrogen molecule, competing with it for a specific receptor site. Nolvadex (tamoxifen citrate) and clomid (clomiphene citrate) are two of the best known estrogen agonists.
- Aromatase Inhibitors: They control estrogen by limiting or preventing the activity of the aromatase enzyme (responsible for converting testosterone and other AAS to estrogen). Femara (letrozole) and arimidex (anastozole) are two of the most well-known aromatase inhibitors.
- Inhibitors of biosynthesis : They control estrogens at their source, preventing their endogenous biosynthesis (which starts with cholesterol through a specific enzyme, in this case the P-450 enzyme system). Cytadren (Aminoglutetimide), Vetoril (Trylostano) and Metyrapone are some of the most commonly used biosynthesis inhibiting drugs. Aminoglutethimide also acts as an aromatase inhibitor.
Estrogen control is essential for health reasons and potential results. Remember that excessive estrogen levels circulating over long periods of time have a negative effect on the heart and other organs due to excess body fat and water retention: increased estrogen = increased aldosterone and water retention. This is why many users appear very “smooth” and puffy (especially on the face) in an AAS flavored cycle.
Young athletes who have not yet reached their maximum physical development should avoid any AAS, especially those caused by premature fusion of the pineal gland.
Note . I have reported on the most common problems experienced by the athlete during the AAS cycle. There are obviously others, but their frequency is much lower and depends on the number and time of hiring. There are also other risk factors associated with misusing other drugs such as GH, IGF-1, insulin, PGF-2, thyroid hormones, etc.
Using blood tests
The main blood tests a Bodybuilder / Athlete should take care of are as follows:
- Liver: LDH, SGOT, SGPT, GGPT, bilirubin, hematological nitrogen (bun), alkaline phosphatase.
- Reni : blood urea nitrogen, sodium, chloride, phosphorus, calcium, potassium, uric acid, CO2, creatine / bun.
- Heart : triglycerides, total cholesterol, HDL cholesterol, LDL cholesterol, HDL cholesterol ratio, HDL cholesterol ratio, potassium, SGOT, SGPT.
- Ossa : calcium, alkaline phosphatase.
- Immune system : GLOBULIN.
- Blood sugar : GLUCOSE.
- Nervous system : POTASSIUM, CHLORIDE, NOD.
There are other, more specific tests that an athlete must perform and these include an overall hormonal picture:
- Total Testosterone
- Free Testosterone
- LH
- SHBG
- estradiol
- Cortisol
- Insulin
- T-3, total T-4 and free
- TSH
- Prolactin
The PSA level is also being studied. it is important. The reference range is usually 0.0 to 0.4 ng / ml. The lower the better. If the levels are high, high DHT and estrogen levels can contribute to prostate cancer. This is a risk, especially in the elderly or people with a genetic predisposition for that matter. There are over-the-counter drugs that counteract the effects of DHT on the prostate gland or hair loss (if predisposed), such as the jagged palm grove.
Obviously, the selection of specific hormone tests should be made at specific times, for example after PCT, to check the level of HPTA axis recovery.
Effective Dosage Factors
For any muscle building chemical to have an effect, you must first set the level above the normal for that person. For example, a man’s normal testosterone production is “about” 35-50 mg per week. That is, the blood level in the blood is 35-50 mg per week. That is, the daily production is from 5 to 7 mg per day. To keep it simple, we assume that 50 mg weekly is the normal blood threshold for a hypothetical Bodybuilder and that blood levels refer to weekly circulating blood levels. For an injection (or oral dose) of AAS to be effective, it must be in an amount that enters the circulatory system at a rate and at a dose that exceeds the normal blood level and therefore the normal blood threshold.
This threshold must be maintained or rise to stay strong. This means that if the AAS used as an example overly suppresses the HPTA function, then this also needs to be compensated by adjusting the exogenous doses.
All AAS and all substances for chemical growth have their own “theoretical” active life. And they all have their own half-lives. The half-life is the time it takes for half of the dose to migrate from the injection site into the vascular system and then disappear. Thus, in theory, a 200 mg dose of injectable testosterone enanthate releases 100 mg over its 4-day half-life, however it remains active throughout its 8-day active life. Thus, testosterone enanthate was administered on the 1st day, and by the 4th day, half of its dose of 200 mg (100 mg) was released, this should exceed the normal level / threshold in the blood, setting a new one, thus causing an effect greater than effect on blood levels. normal. This is what is meant by the term supraphysiological. After several studies of blood tests, it turned out that the drug can have a half-life and active life that is different from person to person, and in different conditions. However, look-up tables exist that include thresholds for multiple doses to determine actual ranges.
Obviously, you cannot specify a fixed value. The lowest dose given as a reference refers to the minimum dose required to achieve an effect. Whereas the higher dose was the point after which another dose did not give better results. In short, there are medications that produce a positive effect of 100 mg, after which the results only improve when doses of 400 mg are reached. To give another example of a cut-off value, 10 mg of Dianabol orally per day produces activity nearly equal to that of human endogenous androgens. Typically, 20 mg of methandrostenolone per day is required to overcome this threshold. Usually for Dianabol, the highest threshold is 5 mg for every 11-12 kg of body weight per day. Learning and previous drug use also greatly affects dosage. A beginner with several years of training experience only needs 2.2 mg per kg of nandrolone decandoate per week to progress excellently on a cycle of just 28 days.
My knowledge tells me that athletes cannot pass any threshold level of a drug before it stops producing acceptable results. This is one of the biggest long-term mistakes that can be seen and which significantly reduces the potential for long-term growth. Natural growth is also the threshold for growth.
Example
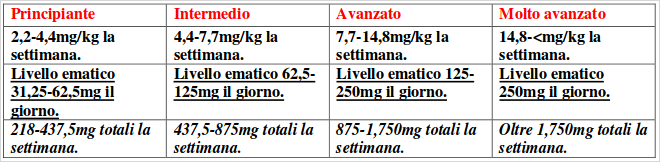
These are general guidelines and assume the following body weights with less than 12% fat :
BEGINNERS : 84-99 kg.
INTERMEDIATE : 99-108 kg.
PERFECT : 108-120 kg .
VERY PERFECT : over 120 kg.
I am repeating a fundamental thing: any effective blood threshold is exceeded before it stops producing results – this is a period of lost growth!
Thyroid hormones, GH, IGF-1 also have minimum effective dosage levels. For example, if the average athlete produces 25 mcg of T-3 per day in order to have the desired effects when taking exogenous T-3, the athlete in question would need to exceed their daily blood threshold (25 mcg); taking a dose of 40 mcg T-3 per day will exceed the threshold of circulating and active blood hormone (action / reaction factors will also act here depending on the time and dose administered).
protocols
The goal of any growth protocol was to gain as much muscle mass and / or lose fat at the same time. This requires a plan to improve, not just maintain or recover from previous cycle losses.
The body has periods and factors of action / reaction. Basically, the body begins to adapt significantly to most attempts to change homeostasis after 2-3 weeks. This is a problem because the cycle usually gives the best results from the 10th to the 30th day. But you can take advantage of this information to benefit the athlete who will use short cycles of 21-30 days (the point at which one or more molecules give the best results) and then walk out of this protocol before negative the side effects outweigh the benefits by entering a different phase / protocol.
Personal experience from in-depth field research tells me that an 8-week cycle that provides a weekly continuous blood AAS level of 400-800 mg, in most cases, begins to no longer produce results throughout the 6th week … This is due to the fact that the level of contrast of the body (overproduction of catabolic hormones, etc.) increases as a reaction to the constant administration of a certain dose of AAS, that is, to the action. Thus, anabolism and catabolism reach almost equal levels. To create a growth environment, one or both of the anabolic / catabolic ratios must be altered in favor of or to increase tissue construction or reduce tissue loss. After 6 weeks, the athlete produces and maintains cortisol levels much higher than normal. Increasing the injected dose will again exceed the cortisol level, but eventually the problem will reoccur. Much worse, when an athlete exits a cycle, high levels of catabolic hormones suppress declining anabolic substances, while HPTA recovery is also far away and most of the cycle gains are quickly lost. It is for this reason that I find it necessary to intelligently structure the protocols throughout the year, which the athlete will have to follow in light of the above.
“Periods of maximum efficacy” of drugs
Now that we have theoretically discussed drug half-life and active life, blood levels and thresholds, let’s now talk about “periods of maximum efficacy.” I understand this may seem like an overwhelming amount of information to consider. But to create protocols that yield maximum results, all action / response factors must be considered. Athletes with better structure (not just externally) do not use the occasional AAS / drugs.
We know that the half-life and active duration of injectable AAS are determined based on the length of the ether chain to which they are associated. The reader should also know why the esterase enzyme acts after injection to induce the migration of free AAS into the vascular system. Any drug introduced into the body by any method has a period of time during which its effectiveness is at best. This is the part of the active life of the drug that gives the best results. It would seem that the drug gives the same effects throughout its active life, but, unfortunately, this is not the case. After the administration of the drug, the esterase enzyme takes some time to act on the ester of the drug and then release it into the vascular system. The longer the AAS ether chain (or any drug), the longer its active life will be. This also means that the migration will take longer. After the drug has migrated into the vascular system, it may take some time for it to become effective. Even if it doesn’t seem, it is not as difficult to see as it might seem.
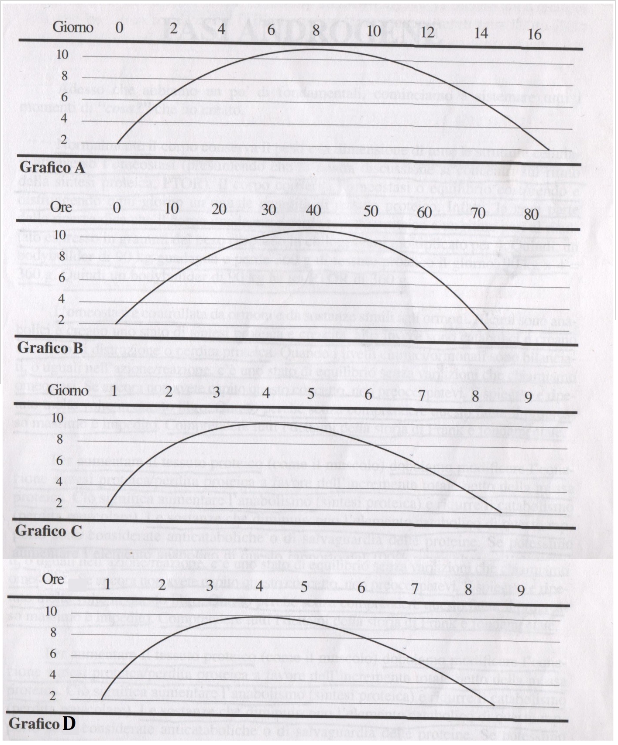
Generally speaking, the period of maximum efficacy of a drug is equivalent to its half-life.
Not the first half of his active life, but usually the central part of his active life. A drug with an active duration of 16 days, such as nandrolone decanoate, will have a maximum efficacy period of about 8 days.
Below are some of the graphing tables I just explained.
Chart A-B-C-D (“Period of maximum efficiency”)
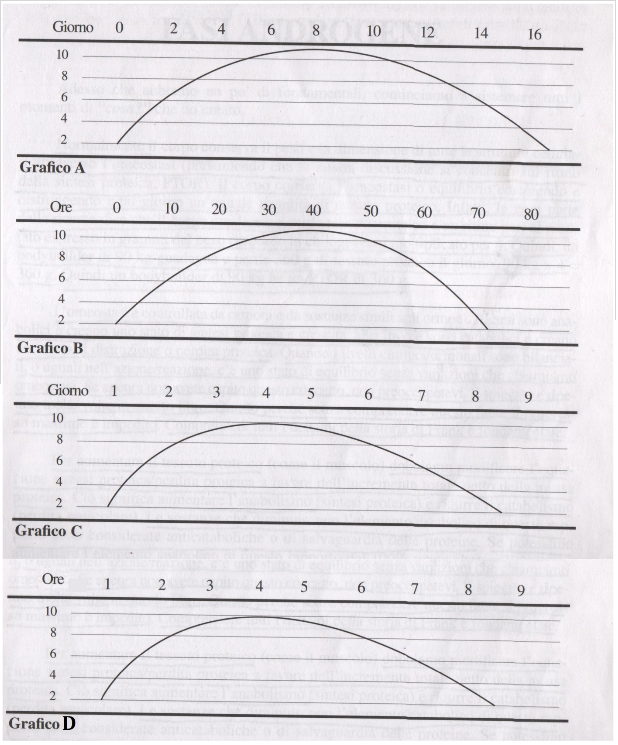
Graph A. This is the period of maximum ether efficiency with an active life of 14-16 days. The drug begins its activity on the 1st day, but shows its true potential from the 4th day. This drug remains in the “period of maximum efficacy” from days 4 to 12, approximately 8 days. Deca-durabolin (nandrolone decanoate), testosterone cypionate and primobolan depot (methenolone enanthate) are in line with this chart.
Graph B . It is a drug with an active lifespan of about 3 days (72 hours). The “period of maximum efficiency” ranges from the eighteenth hour to the fifty-fourth hour. Remember, however, that the drug is also active before and after the “period of maximum efficacy.” This is why it is called an active life. Trends in durabolin and testosterone propionate are consistent with this graph.
Graph C . It is a drug with an active life cycle of approximately 8 days. The “period of maximum efficiency” lasts from 2-3 days to 5 days, that is, about 3-4 days. The trend of Testosterone Enanthate fits this chart.
Graph D . It is an oral drug with an active lifespan of about 6 hours. The “period of maximum efficiency” runs from about 1 to 5 hours. The trend for oral testosterone undecanoate (andriol), dianabol and permobolan is consistent with this schedule.
PCT (Post Cycle Therapy): Restore HPTA and Maintain Lean Body Mass
I often read and hear about people who say that the muscle mass accumulated during the AAS protocols is quickly lost after you stop taking it. However, based on my experience, this was true, but not necessary and preventable for those who knew about the factors of action / reaction of the body. Obviously, water retention, for example due to aromatization, is lost, but the percentage of muscle mass retained depends on how the athlete controls the action / reaction factors.
Inhibiting / decreasing cortisol levels (using Cytadren or PS, for example), inhibiting / decreasing activity and estrogen production (using Femara and / or Nolvadex), and using testosterone stimulants (such as small doses of hCG) can help an athlete recover and retain most of the long term results. Obviously, PCT planning is very subjective, usually even more than AAS cycle planning. However, PCT lasts approximately 4-6 weeks.
Several athletes choose another option: moderate dose AAS replacement therapy (bridge), but check that the overall health range remains positive (hematite lipids, transaminases, hematocrit). Another choice, made primarily by recreational athletes, to maintain gains is to use Ostarina (SARM) between one cycle and the next. This selective androgen receptor modulator does not exhibit significant gonadotropic suppression up to a dose of 25 mg / day. Personally, I would always choose the second option if substitution therapy is not the last option for making progress. However, as mentioned above, PCT should be planned based on specific blood tests.
Findings: Disaster in the Medical Community
Here, I would like to briefly introduce some important recommendations for athletes who intend to launch a chemical integration protocol aimed at improving performance; there would be a lot to add, but at the moment I think that the material that I have put up is more than enough. However, the medical community, carefully selected by multinational pharmaceutical companies, is reluctant to admit the facts are true. With the approval of the Anabolic Steroid Control Act of 1990 (in the United States), there have been dramatic changes in the political climate and in the AAS laws. Unfortunately, this has led to a senseless bias against the medical use of AAS. This demonization of anabolic / androgenic steroids has greatly slowed down the search for inexpensive treatments for the muscle loss often associated with HIV / AIDS. Given that AAS was (and still is) a controlled substance, most clinicians have been and are reluctant to prescribe them for purposes other than those indicated on the label, although AAS may and may offer important health benefits to some of their patients.
– What are the health benefits associated with AAS? –
The combination of AAS and endurance exercise practiced by bodybuilders for decades has shown that many studies can reverse muscle loss and dramatically improve the health and well-being of people with debilitating conditions (such as HIV) and / or sarcopenia. that is, age-related loss of muscle mass. AAS not only reduce and combat muscle loss, they also function as clinically significant modulators of the immune response. The good news is that androgen therapy is gaining respect as a cure for HIV as well as in hormone replacement therapy. Fortunately, I can speak of alternative uses other than those listed on the prescription drug label and classified as AAS (e.g. use of AAS to increase muscle mass, muscle size and strength) .The discussions I have about uses other than those listed on the label are especially necessary and important at a time when social and legal forces threaten the objectivity of the medical community regarding beneficial medical of AAS applications. Fortunately, the use of AAS as a standard medical treatment for muscle loss is gradually gaining acceptance.
Hopefully once again it was helpful to clarify some of the concepts behind chemistry applied to bodybuilding.